Thread by Kevin Bass
- Tweet
- Mar 11, 2023
- #Sociology #ComputerProgramming
Thread
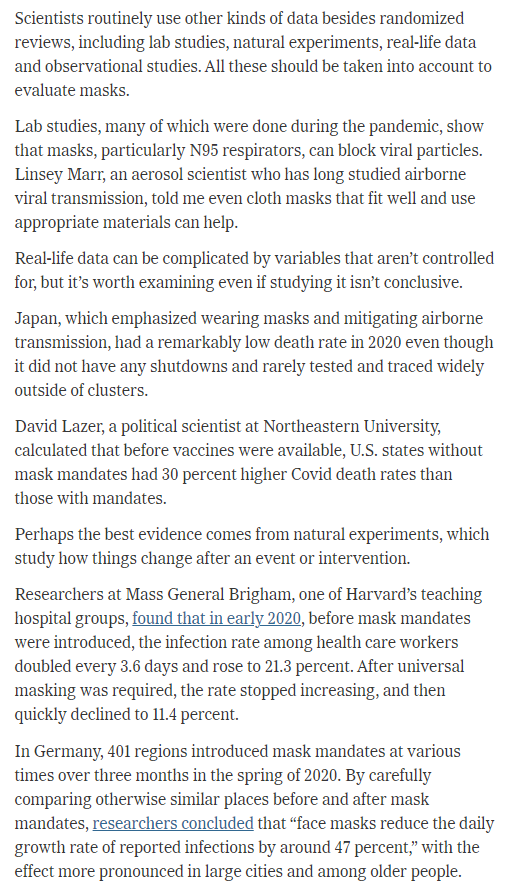
A new op-ed on masks in the @nytimes written by @zeynep, a computer programmer and sociologist, appeared earlier today.
In this thread, I examine and dissect, piece by piece, this op-ed, which is not good.
🧵
In this thread, I examine and dissect, piece by piece, this op-ed, which is not good.
🧵
We'll start with the title.
"Here's why the science is clear that masks work"
Science is clear.
Right.
Let's bear this title in mind. As we shall see, this claim is actually directly contradicted by the text of the article itself.
In other words, it is a lie.
"Here's why the science is clear that masks work"
Science is clear.
Right.
Let's bear this title in mind. As we shall see, this claim is actually directly contradicted by the text of the article itself.
In other words, it is a lie.

The article opens by calling Cochrane a "respected nonprofit", which is not exactly accurate.
Cochrane is the most prestigious medical knowledge synthesis institution on Earth.
This is what @zeynep in her @nytimes op-ed is purporting to debunk.
Let's see how she does.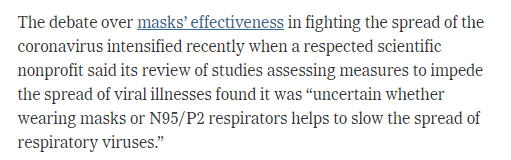
Cochrane is the most prestigious medical knowledge synthesis institution on Earth.
This is what @zeynep in her @nytimes op-ed is purporting to debunk.
Let's see how she does.

@zeynep starts by pointing out that the review was unclear in its summary, and misinterpreted.
It doesn't show that "masks don't work", she says.
But just as @zeynep (along with Cochrane's editor-in-chief) disagrees with this interpretation, I disagree with theirs.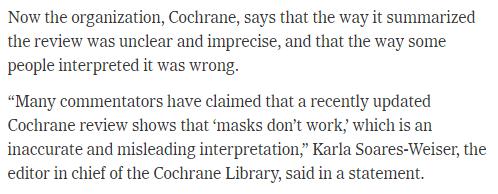
It doesn't show that "masks don't work", she says.
But just as @zeynep (along with Cochrane's editor-in-chief) disagrees with this interpretation, I disagree with theirs.

I think the review effectively *does* show that masks do not work, but we do have to qualify what we mean by that precisely.
We'll get there. But let's keep following the text.
We'll get there. But let's keep following the text.
The essay then transitions to a core point used by pro-maskers: the Cochrane collaboration only examines mask RECOMMENDATIONS, not mask-wearing itself. 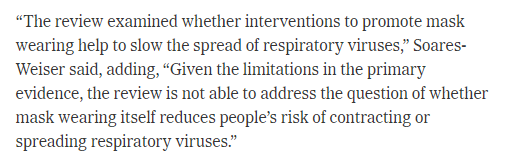

This move allows pro-maskers to say that, yes, the randomized controlled trial literature cannot find much of an effect of mask recommendations, but that's only because of low adherence. If adherence was higher, then the effect would show up, because MASKS WORK.
This distinction and argument needs to be closely examined, because I think it is conceptually incoherent and scientifically indefensible.
It is in my opinion a kind of pseudoscience.
I will demonstrate why with an example.
It is in my opinion a kind of pseudoscience.
I will demonstrate why with an example.
Say you are running a cancer drug clinical trial. You have a group of patients assigned to take a placebo (sugar pill) and another group assigned to take your cancer drug. The trial lasts, let's say, for 12 weeks.
Unfortunately, there is a problem
Those assigned to take the cancer drug find it so unpalatable and bitter, and so impossible to take on a daily basis, that they stop within the first few days.
Only 1-in-5 patients take the drug.
Those assigned to take the cancer drug find it so unpalatable and bitter, and so impossible to take on a daily basis, that they stop within the first few days.
Only 1-in-5 patients take the drug.
Now that 20% does pretty well. They outperform the placebo group.
However, on average, there is no statistically significant difference between the group assigned to take the drug (remember that 4-in-5 patients don't take the drug) and the group assigned to take the sugar pill.
However, on average, there is no statistically significant difference between the group assigned to take the drug (remember that 4-in-5 patients don't take the drug) and the group assigned to take the sugar pill.
Does the pill work?
Well, what if we only compare the 20% of those adherent to the placebo? Then couldn't we determine if the pill works?
Well, what if we only compare the 20% of those adherent to the placebo? Then couldn't we determine if the pill works?
Not so fast. Because that 20% that was adherent, it turns out, were much healthier at baseline, much more robust, and more likely to survive in the first place. That's why they were able to take the pill. They had more strength to gut it out every day, so to speak.
So is there something special about people who adhere that accounts for their better outcomes than the placebo group?
Or is it the drug?
The fact is, we don't know. Because now the study is confounded.
Or is it the drug?
The fact is, we don't know. Because now the study is confounded.
Thus, if adherence is not high enough, it's simply not possible to compare the drug to the sugar pill.
Because if not enough patients take the drug, the treatment effect gets washed out by the patients who don't take it.
Because if not enough patients take the drug, the treatment effect gets washed out by the patients who don't take it.
And we cannot analyze the patients who do take it separately without introducing bias.
(This kind of analysis, for the record, is called a per-protocol analysis, and is well-known to have this bias and is not considered definitive for the reason I discussed.)
(This kind of analysis, for the record, is called a per-protocol analysis, and is well-known to have this bias and is not considered definitive for the reason I discussed.)
And here we land on a critical point: in such a case, we cannot then conclude that the drug works if only people would take it.
That's actually a fallacious conclusion.
In reality, we don't know, because we were never able to test our hypothesis due to low adherence.
That's actually a fallacious conclusion.
In reality, we don't know, because we were never able to test our hypothesis due to low adherence.
Now what pro-maskers want to do is they want to say, "OK yes, the randomized controlled trials that recommend masks don't show much impact of masks, but we know that masks work anyway."
Here's the big question: how?
Here's the big question: how?
@zeynep alludes to that here. We will discuss that in a moment.
If the trial where they recommend masks doesn't work, how do they know if masks themselves work?
We shall return to this later. Because it's quite the snag.
We shall return to this later. Because it's quite the snag.
But this isn't the only problem. There is actually a much, much, MUCH bigger problem that pro-maskers avoid talking about here.
And that's this...
And that's this...
If the pro-maskers concede that randomized controlled trials recommending masks never show much of an effect because of low adherence, then they're conceding that we simply do not know of any way to recommend masks to make them work on a population level.
That is to say, even if pro-maskers were to save masks in this way, by insisting that masking itself works but masking recommendations don't, then they concede that as a public health intervention, given current methods of promoting mask-wearing, mask recommendations are useless.
What we are left with, for pro-maskers, is a useless public health intervention on a population level, but a potentially useful, individual-level biohack.
Mandates are out of the question.
Mandates are out of the question.
That's right, on this interpretation, rather than promoting some sort of public health intervention, @zeyneb is promoting some sort of biohack in the New York Times.
"Try and see if it works for you!"
This is what we are reduced to.
With zero relevance to public health.
"Try and see if it works for you!"
This is what we are reduced to.
With zero relevance to public health.
Think about this more deeply. If randomized controlled trials recommending masks don't work, then why should an op-ed New York Times recommending masks work?
This reduces even the @nytimes piece to a kind of idle mental gymnastics that, itself, is very unlikely to produce any meaningful benefit in the readership.
It is just a signaling game, according to the overwhelming evidence.
And quite the signaling game it is. Indeed, indeed.
It is just a signaling game, according to the overwhelming evidence.
And quite the signaling game it is. Indeed, indeed.
In any case, you now understand the layout of the scientific issues.
Let's slide back to the text.
@zeynep then quotes the EIC of Cochrane again, as disagreeing with the lead author of the review.
Again, I disagree with them both for reasons I will discuss in a moment.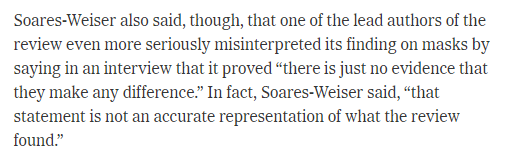
Let's slide back to the text.
@zeynep then quotes the EIC of Cochrane again, as disagreeing with the lead author of the review.
Again, I disagree with them both for reasons I will discuss in a moment.

Zeynep then introduces the concept of meta-analysis and points out that the low adherence undermined the conclusiveness of the study results. 

She then again complains that in most of the studies included, there was low adherence. 



She finally gets to a study she approves of, which shows reduced spread if the mask was worn consistently.
But she doesn't include all of the details.
But she doesn't include all of the details.

The study actually failed to meet its primary endpoint due to lack of adherence, and investigators had to slice the study up to find significant results somewhere.
@zeynep doesn't share that though.
bmcinfectdis.biomedcentral.com/articles/10.1186/1471-2334-12-26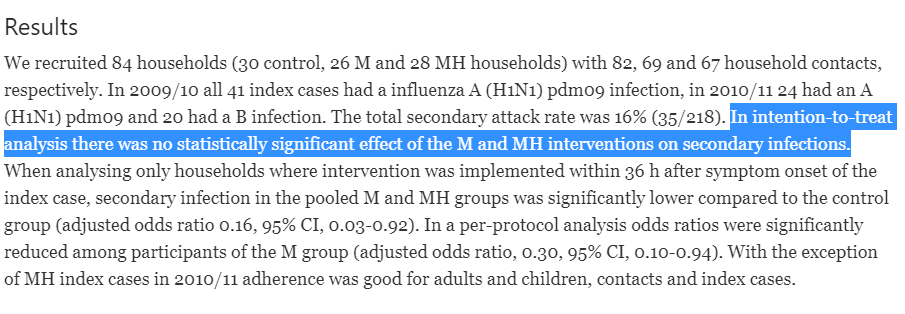
@zeynep doesn't share that though.
bmcinfectdis.biomedcentral.com/articles/10.1186/1471-2334-12-26

@zeynep then mentions how the Cochrane EIC worried that the reception of the review--as showing that masks don't work--might undermine the collection of data in the future. 

Quite interesting, since the headline for this op-ed, which is a lie, should achieve the same result: persuade readers that the mask issue is settled and resolved. Hence no need for more detail.
Ironic indeed.
Ironic indeed.

@zeynep continues with the canard that there is a distinction between whether a mask reduces a wearer's risk and whether recommendations reduce infection in a community.
As we have already seen, this distinction promises to save masks but gives us only rocks.
As we have already seen, this distinction promises to save masks but gives us only rocks.

Finally Zeynep settles on the Bangladesh trial.
She mentions the modest 11% reduction in COVID cases.
What she doesn't discuss is this re-analysis that attributes this finding to bias, reanalyzing the data and finding no benefit.
trialsjournal.biomedcentral.com/articles/10.1186/s13063-022-06704-z
She mentions the modest 11% reduction in COVID cases.
What she doesn't discuss is this re-analysis that attributes this finding to bias, reanalyzing the data and finding no benefit.
trialsjournal.biomedcentral.com/articles/10.1186/s13063-022-06704-z

@VPrasadMDMPH threads this trial here:
More adherence issues. 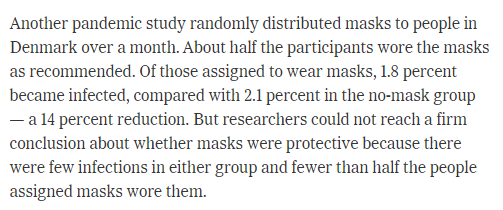

Here Zeynep makes the claim that it would have been unethical to have run randomized controlled trials to test masks, which have pretty consistently not worked in randomized controlled trials. 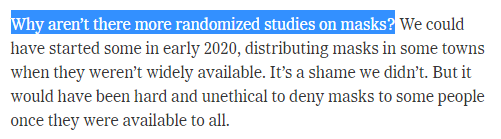
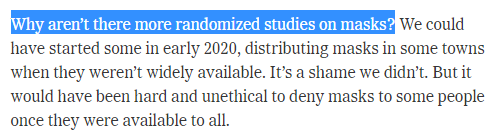
That's funny. How can something that has never worked in randomized controlled trials be unethical to withhold in a randomized controlled trial? One would think that only effective treatments would be unethical to withhold.
Must have missed this one in my ethics classes.
Must have missed this one in my ethics classes.
Remember that we still needed to have some kind of evidence that masks work, at least for their wearer, if not in randomized controlled trials?
Zeynep comes through and marshals the evidence.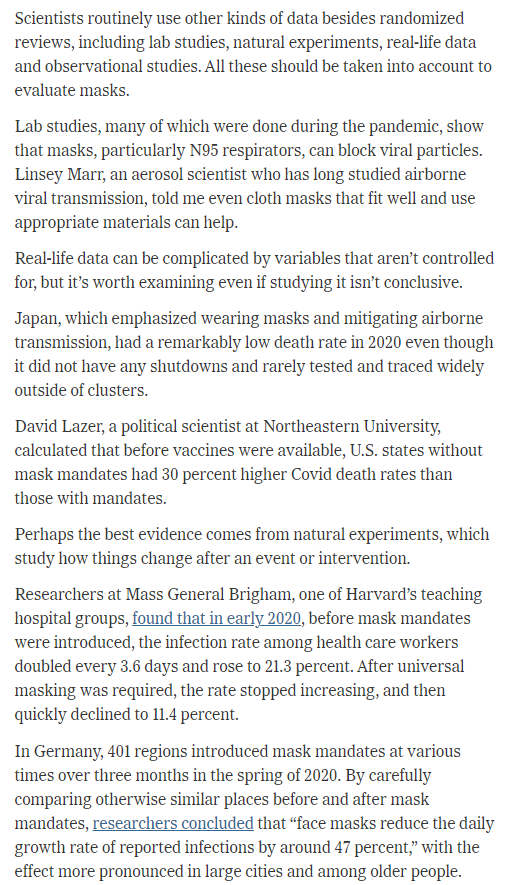
Zeynep comes through and marshals the evidence.
The only problem? This same level of evidence "proves" that the following medicines also work to treat COVID:
Hydroxychloroquine
Ivermectin
Vitamin D
Curcumin
Elderberry
Ginseng
Magnesium
Zinc
Melatonin
Fish oil
Quercetin
NAD boosters
Selenium
Vitamin C
Vitamin E
Hydroxychloroquine
Ivermectin
Vitamin D
Curcumin
Elderberry
Ginseng
Magnesium
Zinc
Melatonin
Fish oil
Quercetin
NAD boosters
Selenium
Vitamin C
Vitamin E
And countless others.
When you decide to "fall back" to evidence that is not in a randomized controlled trial, everything works! Including masks! Amazing!
When you decide to "fall back" to evidence that is not in a randomized controlled trial, everything works! Including masks! Amazing!
And now let's also revisit my strong claim that the Cochrane review shows that "masks don't work." If we take a look at the above list, virtually none of those treatments work.
And that's the idea: until something has been proven to work in a randomized controlled trial, its probability of working is near zero. This is because the vast majority of clinical hypotheses turn out to be false.
In other words, all plausible but unproven therapies are assumed to not work until they are shown to work, an assumption that will be born out 99 times out of 100.
That is what is meant when I (or Tom Jefferson) say that "masks don't work."
I am almost certainly right; I know this before any data whatsoever are presented before me, and am surprised if positive data does show anything to work.
Because in medicine, almost nothing does.
I am almost certainly right; I know this before any data whatsoever are presented before me, and am surprised if positive data does show anything to work.
Because in medicine, almost nothing does.
Let's summarize.
To save masks from oblivion, pro-maskers distinguish between mask recommendations and masks themselves.
This distinction fundamentally undercuts masks as a public health measure and establishes them as, basically, an individual-level biohack.
To save masks from oblivion, pro-maskers distinguish between mask recommendations and masks themselves.
This distinction fundamentally undercuts masks as a public health measure and establishes them as, basically, an individual-level biohack.
Furthermore, to even maintain "masks themselves" as viable, non-RCT data has to be fallen back on, which means the same level of data that shows that virtually every other treatment works, including ivermectin, hydroxychloroquine, quercetin, etc.
This is what Zeynep's argument amounts to: absolutely nothing.
To add that cherry on top, @zeynep finishes by a bold appeal to authority.
A doctor she interviewed is "very confident"!
Bravo!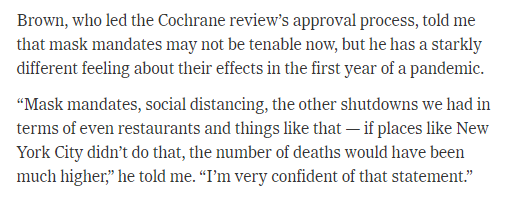
A doctor she interviewed is "very confident"!
Bravo!

@zeynep celebrates her victory: "So the evidence is relatively straightforward." 

She continues to add details, as if she was merely summarizing what she had already said, that nonetheless weren't discussed up to this point:
"Consistently wearing a mask, preferably a high-quality, well-fitting one, provides protection against the coronavirus."
"Consistently wearing a mask, preferably a high-quality, well-fitting one, provides protection against the coronavirus."

?????????
@zeynep then discusses some irrational reasons why people are opposed to masking
Then she makes the concession: "Some mask proponents and public health authorities have also used weak studies to make overblown or imprecise claims about masks’ effectiveness."
Bruh.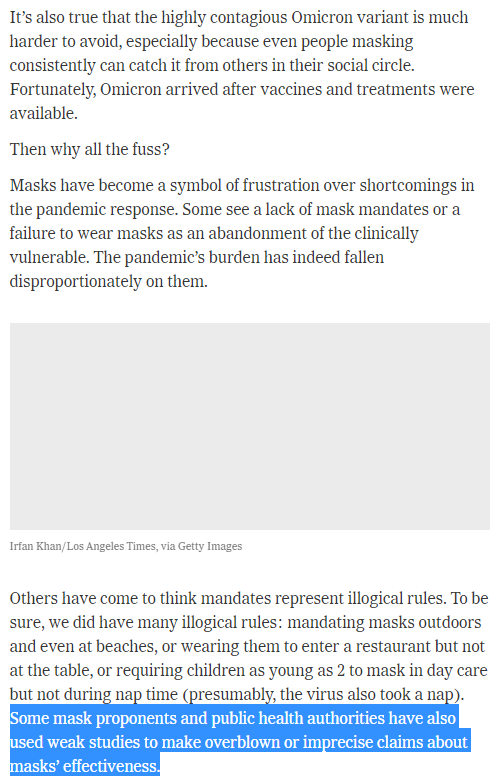
Then she makes the concession: "Some mask proponents and public health authorities have also used weak studies to make overblown or imprecise claims about masks’ effectiveness."
Bruh.

Zeynep then engages in some ad hominem against Tom Jefferson, the lead author of the Cochrane review. 

Finally, Zeynep calls for us to "continue to collect data on mask wearing, despite the challenges".
One wonders why such data collection would be necessary, since wasn't the title of the article: "Here’s Why the Science Is Clear That Masks Work"?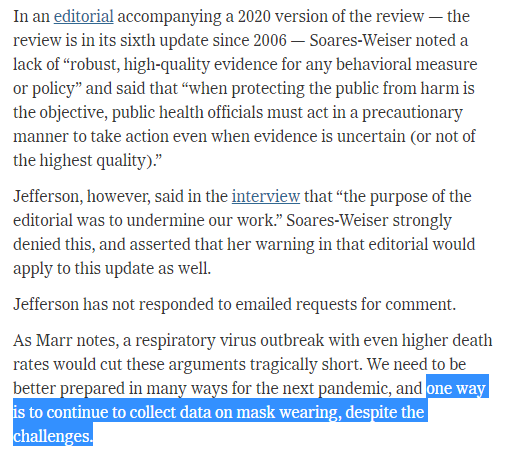

One wonders why such data collection would be necessary, since wasn't the title of the article: "Here’s Why the Science Is Clear That Masks Work"?


????????
One also wonders how it is possible to even collect data and conduct randomized controlled trials when, as we saw, it was unethical to not give some people masks, which have never been shown to be effective, when there are enough masks for everyone.

If you enjoyed this thread please click the bell icon next to the follow button until it shows a checkmark. It should look like the image below.
This will send you notifications whenever I post something new.
This will send you notifications whenever I post something new.

Also check out my COVID substack!
Subscribe for free
And become a paid subscriber if you find my content valuable
covidcommentary.substack.com
Subscribe for free
And become a paid subscriber if you find my content valuable
covidcommentary.substack.com
ADDENDUM
I suspect that the distinction between "masks themselves" and "mask recommendations" is based on a moral judgment about the value of masks: the reason that masks haven't been found to be effective is that the study participants were not moral.
I suspect that the distinction between "masks themselves" and "mask recommendations" is based on a moral judgment about the value of masks: the reason that masks haven't been found to be effective is that the study participants were not moral.
It's similar to the way that diet zealots look at diet studies. When subjects are not adherent to the diet, the diet is not blamed. The participants are. "It's not a problem with the diet. The study participants just did it wrong."
This is at odds with the way public health and science are normally taught, and is also at odds with patient-centered care in medicine. For maskers, study outcomes can be rejected because morality trumps the facts.